Saturday, 13 June 2015
EHA 2015- learning from patient advocates in hematological cancers
Very honoured to have been invited to give a talk in the patient advocacy track at EHA 2015 in Vienna- on risks in innovative trial designs, so a topic very close to my heart :-).
The PA community in hematological cancers- notably in CML and Myeloma- has been and still is of great help to MPNE as we can learn a lot from organisations that have been around for considerably longer than us.
The first advocacy session was on patient participation in clinical research- the first speaker had a great online tool how to capture audience preferences via a webbased tool- something to take up :-): http://PollEverywhere.com - and was a clinician who shared how he got patients responses to take that to discussions with his ethics committee for his clinical trials.
Very revealing for me was the question about information about the results of the trials- patients overwhelmingly wanted to get informed about the results of the trial personally via email or SMS- while the ethics committee insists on protecting the anonymity of the trial participants was in the main interest of trial participants. MHMMMM.
Jan Geissler from the CML advocates network spoke about patients participating in clinical research and my talk was on the perceived risk associated with new drug development models like adaptive licensing- the presentation will be shared on the MPNE fb forum.
Douwe then presented the results from the EMA risk/ benefit assessment tool, one part of the data coming from the last MPNE 2015, the other from the conference of Myeloma Patients Europe!!!
The data is still insufficient for the sub-groups but that is definitely something for us to take up and great to hear that our data is useful for such a project! So happy :-)
In the second session, Ananda Plate from Myeloma Patients Europe (MPE) spoke about the Atlas on Access to Myeloma treatment, an MPE project where they got European Myeloma groups to collaborate to find out which drugs are available and which ones aren't - and the need for us as advocacy community to work together strategically and to get more candid about generating the necessary data to have evidence to support our demands.
H. Ludwig, a clinicians, gave a very open talk about the pricing and healthcare budget impact of new drugs- the Ipi/ Nivo combination in Melanoma was mentioned as a very familiar example to us. And he ended by suggesting a Pan-European buying syndicate to negotiate for better prices Europe-wide.
G Constantinou from the Thalassaemia International Federation made a very good comment on quality of life 'I don't want to have a treatment that gives me a quality of life just good enough to get me back to hospital'. Very true indeed.
Organisations to follow
http://www.cmladvocates.net
http://www.myeloma.org.uk
http://www.mpeurope.org
Saturday, 2 May 2015
Dying for evidence- no thank you.
Dear author,
http://www.bmj.com/content/350/bmj.h2068
please let me assure you- cancer is very much the evil and invincible predator you describe.
As I got to experience first-hand when I saw my husband die extremely painfully from Melanoma, only 15 days after his 37th birthday. I will never forget the relief when the tumours finally distroyed the nerves in his pelvis- the paralysis was nothing compared to the fact that we could reduce the morphines to a a degree that he was awake and we got a few more precious hours to talk before he slipped into a coma never to wake again.
You could also ask my youngest daughter- she was 4 at the time- what death from a combined liver/ kidney failure looks like, her recollection of seeing her father die is very accurate. Or you could ask my older daughter- although I am not sure she remembers that she climbed on to her father's bed just after he died to tightly hug him- we hadn't been able to do that for the last weeks as any touch had become too painful.
Before his death, my husband had taken part not in one but two clinical trials, plus an early access program- something most fervent promoters of the hardest lines of evidence will never be able to claim about themselves.
The first trial he participated in would probably have been very much to your liking and perceived high quality standards, considering it was randomized, although not blinded. Yet, undergoing the randomisation for this trial qualifies as one of the worst experiences of my life- just up there with him receiving a Stage IV Melanoma diagnosis without any prior warning and then, his death.
Why?
At medical school, I had been infected by the virus of evidence-based medicine- I remember very clearly sitting in the lecture theatre (lower part on the right) and the relief that there was a way to actually protect my future patients from my own lack of experience- one of the deep-seated fears any medical professional I know has, especially at the beginning of their career.I then went on to a lab-based training in Molecular Biology, with serious emphasis on scientific rigour and the need for appropriate controls- I thought I knew what good science was about.
Now, on the other side, being subjected to the evidence-generating part of this brave new world of evidence-based medicine, my husband all of a sudden risked being randomized to a clearly inferior control arm.
This is what one of our patients said in a very similar situation:

(you can watch her story here, including her oncologist's reaction when she decided to make use of her right to withdraw from the trial. He would only refer her to the next center if she accepted any treatment she was randomised to)
Now,
Melanoma is a very specific case. After years of no therapeutic progress, we all of a sudden have not one but two classes of therapies available. As based on insight into the underlying molecular mechanisms, these drugs present considerable advances over the previously existing 'gold'-standard of chemotherapy, DTIC- rather to be considered a standard of desperation and medical actionism but definitely not golden. (At the same time, I learned about evidence-based medicine, I also learned the Melanoma was both resistant to chemo and radiotherapy, so this is hardly news).Yet, every single Melanoma drug we have had in the past few years has been tested in a clinical trial against DTIC- the last example that led to a positive recommendation by the European Medicines Agency only last week can be found here.
Extract:
'After 12 months, the survival rate of patients treated with Opdivo was much higher than the rate of patients who received dacarbazine (73% compared with 42%).'
Originally,
the motivation for randomized controlled trials (RCTs) was to deliver clinically relevant information and to provide insight in situations where there was clear uncertainty, not to produce statistics for statistics' sake.A Phase 3 study delivering a result where one arm has nearly double (1.7 to be precise) the survival than the other arm allows for 2 possible conclusions:
1. The enormous difference was not picked up in the previous Phase 2 study. Which raises serious doubts about the professional capabilities of the parties involved.
2. The difference was clear when the trial started. Which makes this an equipoise-violation from day 1, violating the principles clearly stated in the Helsinki declaration - among them the binding declaration of physicians 'The health of my patient will be my first consideration'.
As a patient, neither choice is acceptable.
So the argumentation of this article falls in my opinion short on several levels-
1. Failing to recognize the diversity between the development in different cancers. Incremental progress in the past in one cancer should not kill patients in the process of evidence-generation in a different cancer at present. Tools need to evolve with scientific progress.
2. Mistaking statistical significance for clinical relevance. From a clinical point of view, it is irrelevant whether a new drug is 71%, 72.5% or even 75%- in the Melanoma example above, it is 73.8%- better than the previous standard as a patient will be getting the new therapy anyway.
3. Failing to recognize the limitations of and alternatives to randomized clinical trials. RCTs are designed with optimal comparability between groups (and favourable outcomes for the sponsor) in mind, not with representativeness with respect to the disease. In Melanoma, this concretely meant that patients with brain metastases were systematically excluded from clinical trials for a very long time. In a disease where cerebral involvement is the major driver of mortality and 80% of our patients have metastasis to the brain at death, this raises serious doubts about the clinical relevance of such a design.
On the other hand, alternative designs are available but not widely used- Bayesian trial designs e.g. allow to minimise the risk to expose patients to inferior treatments but are statistically more demanding. Having said that, certainly a patient's life is worth the effort?!
Increasingly, HTA bodies and payers demand data on effectiveness to see how a new drug performs in the real world, not only in an idealised/ inappropriately optimised setting. Currently, systematic data gathering after the approval of a drug focuses on the safety aspects of a new medication, neglecting the potential benefits- the faster we generate evidence into how and when to use new medication, the better for all of us.
4. An unhealthy amalgam of evidence and price. If new cancer drugs were available at a quarter of the current price, this discussion would in all likelihood be mute. While even CEOs of large pharmaceutical cooperations recognise that the current price level is unsustainable- to quote Jimenez, Novartis CEO, from his interview with Forbes:
'What you know is not going to happen is the ability to stack therapies on top of each other at the current price and expect people to pay,” he says. “ The whole oncology pricing structure needs to be rethought because it’s reached the level that is not going to be sustainable for the long term.'
health care systems now use evidence- or rather the lack thereof- in order to negotiate for better prices. The call for more evidence in justification for outrageous drug prices provides a short-term negotiation advantage but then paradoxically increases the costs of the development even further, contributing to the very effect it was intended to control.
While the current system is clearly financially unsustainable, we have no societal contract in place stipulating that patients should die in order for the health care system to negotiate for better drug prices. Effectively, this means that with the diagnosis, a patients looses parts of his or her right to live.
The right to live is one of our fundamental human rights- which effectively turns a trial like the one mentioned above into a human rights' violation. Not to mention that the costs for drugs amount to around 10% of the healthcare spending in developed countries and one could argue that healthcare systems are conflicted as e.g. investments to reduce administrative costs or diagnostic redundancy are harder to implement and do not deliver the same short-term positive budget impact as a saving in drug spending.
5. Logically following on to that and to preempt the point that patients are not forced to take part in clinical trials. In a disease like Melanoma, the most promising new drugs offering the best chance of survival are still in clinical development, the standard of care for stage IV Melanoma is therefore still clinical trial participation. Arguing that a patient actually has a 'choice' to rather die on the standard of care instead of entering a clinical trial with a potentially life-saving drug is cynical. In many diseases, clinical trials ARE treatment and for our patients, clinical trials are part of their treatment strategy.
6. Inaccurate temporal perception. Patients need to take treatment decision at a single point in time, so the perception that 'we just need to accumulate more evidence and then treat the patient in an optimal fashion' is incorrect- because that very patient will in all likelihood be dead or past the ideal time point of treatment. This process is also too slow, especially in fast-progressing diseases like Melanoma where the historic survival after a Stage IV diagnosis was 6- 9 months, failing not only today's but also tomorrow's patients.
So instead of letting patients 'die in safety', we need to invest more efforts into processes like adaptive licensing which grant earlier access to a wider patient population while systematically gathering evidence- this will deliver better data faster and hopefully also in a more cost-effective way.
It's time for the 21st century
And last but not least- are processes like randomisation, blinding and placebo-use actually still considered ethical in the 21st century? Or are they rather the remnants of the paternalistic concepts of clinical medicine of the last?
In the end, it is up to the individual patient to decide.
As the Helsinki declaration clearly states in Article 8:
'While the primary purpose of medical research is to generate new knowledge, this goal can never take precedence over the rights and interests of individual research subjects.'
Patients are full members of our societies, tax-payers, voters and contributors to our healthcare systems. And they are increasingly insisting on their rights- or directly taking it into their own hands.
We need a broader discussion in society how to provide sustainable healthcare in the future for all of us and high-level strategies instead of short-term fixes for innovation- and accountability for the losses of lives caused by the current system.
Above all, we need ways of generating high quality, clinically relevant evidence in a cost-effective way that does not kill our patients in the process because the ultimate question remains:
Would you want to be the patient on one of these trials?
Bettina Ryll
Melanoma Patient Network Europe
http://www.melanomapatientnetworkeu.org
Declaration of interests:
Bettina has lost her husband to Melanoma in 2012 and since then, several friends. All of them died a horrendous death and all of them had participated in clinical trials.
Currently, she holds a researcher position in Evolutionary Biology at Uppsala University.
She founded the Melanoma Patient Network Europe in 2013 and her special interest is patient centric clinical trial design. In that capacity, she interacts with different stakeholders- the pharmaceutical industry, research societies, EMA and HTA bodies.
Currently, the basic costs of the Melanoma Patient Network are covered by Bettina's honoraries for advice/ consultancy/ talks; currently she does not receive a personal salary nor any remuneration for her work at MPNE.
Conferences and meetings are predominantly covered by unrestricted grants by the pharmaceutical industry, balanced between companies with competing interests in Melanoma, and without any influence on concept, faculty or other. Project work with e.g. EMA or GetReal was covered by the respective project partner.
More information on MPNE's activities can be found on the MPNE website.
Friday, 1 May 2015
We are not that stupid! The difference between lay language and inaccurate data representation.
Today, I read this really unhelpful publication entitled
Clinical Trial Data Transparency: The Dangers Of "Putting It In Layman's Terms
which without getting into the details of the disease- yet another time- promotes some major and recurrent misconceptions about patients.
1. 'Lay language means inaccurate'.
Just because you are not allowed to use jargon or abbreviations does not give you permission to cheat or misrepresent data to your own advantage. That's called 'scientific fraud', not 'lay language'.
2. 'Patients are inherently stupid'.
Diseases hit a crosscut of society and no, you do not loose your brain nor your education when being diagnosed with a serious condition. Plus, some patients spend considerable amounts of time educating themselves so believing that patients 'just don't get it' is- naive.
3. 'Patients don't get risk'.
The diagnosis with a serious condition, especially a life-threatening cancer, changes your perspective on everything- including on what is truly risky in life. Similarly to not having a clue what it's like to have kids before having your own first one. The comparison also holds true for the advice you gave as a childless person to your friends with kids- useless at best, more likely dead-embarrassing. But you'll only know once you get to the other side….
4. The link between evidence and time.
Patients often need to take decisions at a single point in time, so cannot simply sit around for some elusive evidence to accumulate. Because, if you e.g. have Melanoma you'll be dead by the time most healthy individuals are pleased with the available level of evidence. That's then called 'dying in safety'.
So lay language has nothing but absolutely nothing to do with the misrepresentation of data!!!
Wednesday, 4 February 2015
Word Cancer Day- Our time is now
World Cancer Day
Melanoma and Myeloma are very different cancers- although people mix us up often enough as they sound so similar- but what Alfonso from Myeloma Patients Europe has to say also applies to us in Melanoma!
OUR TIME IS NOW.
'We're slowly and progressively winning the battle against cancer. However, there's still lot to do, and it is the time for patients to become more active and empowered in research, policy-making, education and awareness. Today, 4th of February, World Day Against Cancer, is a good chance to remember and encourage ourselves to keep committed to face this challenge. It is our time now.'
Alfonso Aguarón from http://www.mpeurope.org
Wednesday, 7 January 2015
Tuesday, 6 January 2015
50 years of B lymphocytes and why it matters for Melanoma
Immunology: Fifty years of B lymphocytes
http://www.nature.com/news/immunology-fifty-years-of-b-lymphocytes-1.16653
In 2013, Cancer Immunotherapy was chosen as the breakthrough- therapy of the year 2013 by the scientific journal Science, a choice Melanoma patients can relate to very well- as it is novel anti-based therapies blocking brakes in the bodies own immune system- like CTL4, PD1 or PDL1 antibodies- that for the first time ever provide substantial hope of long-term survival in Melanoma.
The article in Nature at the occasion of the 50th anniversary of the publication of the paper that first described two classes of lymphocytes- without this knowledge, we wouldn't have today's greatest hopes in Melanoma.
From the article-
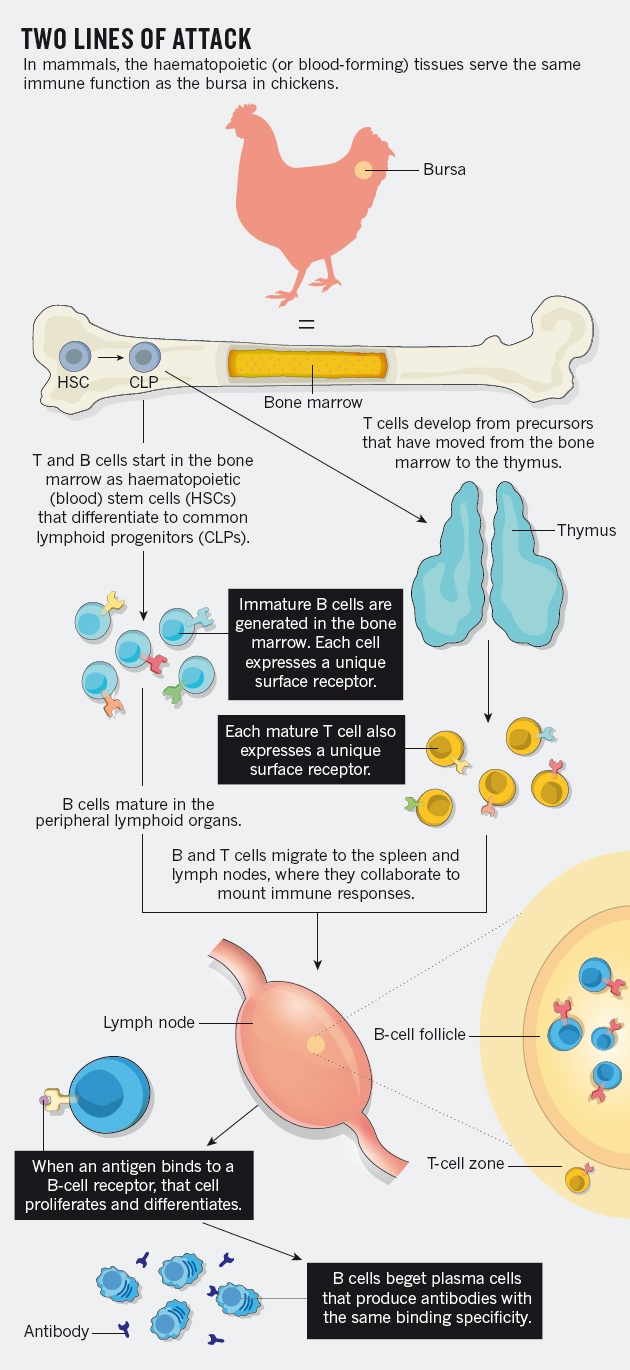 'At the time, the central question in immunology was how vertebrates tailor their defences to bacteria and viruses, whose chemical structures show nearly unlimited diversity. Within two years of joining Good's laboratory, Cooper had made a discovery about the cells that accomplish this task — lymphocytes — that proved essential to cracking the mystery, and ultimately to unifying the camps of his field.
'At the time, the central question in immunology was how vertebrates tailor their defences to bacteria and viruses, whose chemical structures show nearly unlimited diversity. Within two years of joining Good's laboratory, Cooper had made a discovery about the cells that accomplish this task — lymphocytes — that proved essential to cracking the mystery, and ultimately to unifying the camps of his field.
Fifty years ago this week, Good, Cooper and their colleague Raymond Peterson published a paper1 in this journal revealing that there are two types of lymphocyte. The insight shaped the course of modern immunology and influenced the study and care of immunodeficiency conditions, cancers of the immune system and the development of monoclonal antibodies — powerful research tools and therapeutics.
…. read further here
p.s. considering the amount of tax-funded research that went into these discoveries over now more than 50 years, maybe society should be getting a better ROI in form of affordable drugs?
Saturday, 27 September 2014
Banning patient advocates from parts of congresses is unconstructive and anachronistic.
The ultimate purpose of medicine is to serve patients.
Only
patients can tell us whether a treatment meets their expectations. In these
exciting times, where break-through discoveries meet financial austerity,
ignoring patients’ demands is a waste of resources that we as civil society
should not tolerate.
Patient advocates are de facto health care professionals,
providing patients with support, advice and information. It is therefore in all
our interest that advocates have access to reliable, validated information
sources and are as educated as possible to
1. best serve patients and
2.
contribute the patient perspective in a maximally constructive way, so that we
are reaching our goal- meaningful medicine for all patients.
The current situation at the ESMO 2014 congress where
advocates are banned from certain areas of the conference is therefore both
unconstructive and anachronistic. The very same advocates meant to require
protection from the- highly regulated and checked for scientific and legal
accuracy- promotional material for new drugs have already discussed the
clinical trial protocols and set on the advisory boards when these very drugs
underwent development.
Patient advocates attending scientific congress are highly
motivated individuals who dedicate enormous amounts of their time- often
unpaid- to educate themselves in order to help others. We as society ignore
that expertise at our own peril.
Today, it is opportune for everyone in health to claim to have 'the patient at the centre' of all endeavours. For all of us as society to profit from the existing patient knowledge to build a better future, not only for today's but also for future patient generations, will require more than lip service.
Bettina Ryll
Founder Melanoma Patient Network Europe

Subscribe to:
Posts (Atom)